Unfortunately Ausmed.com does not support your browser.
Please upgrade your browser to continue.
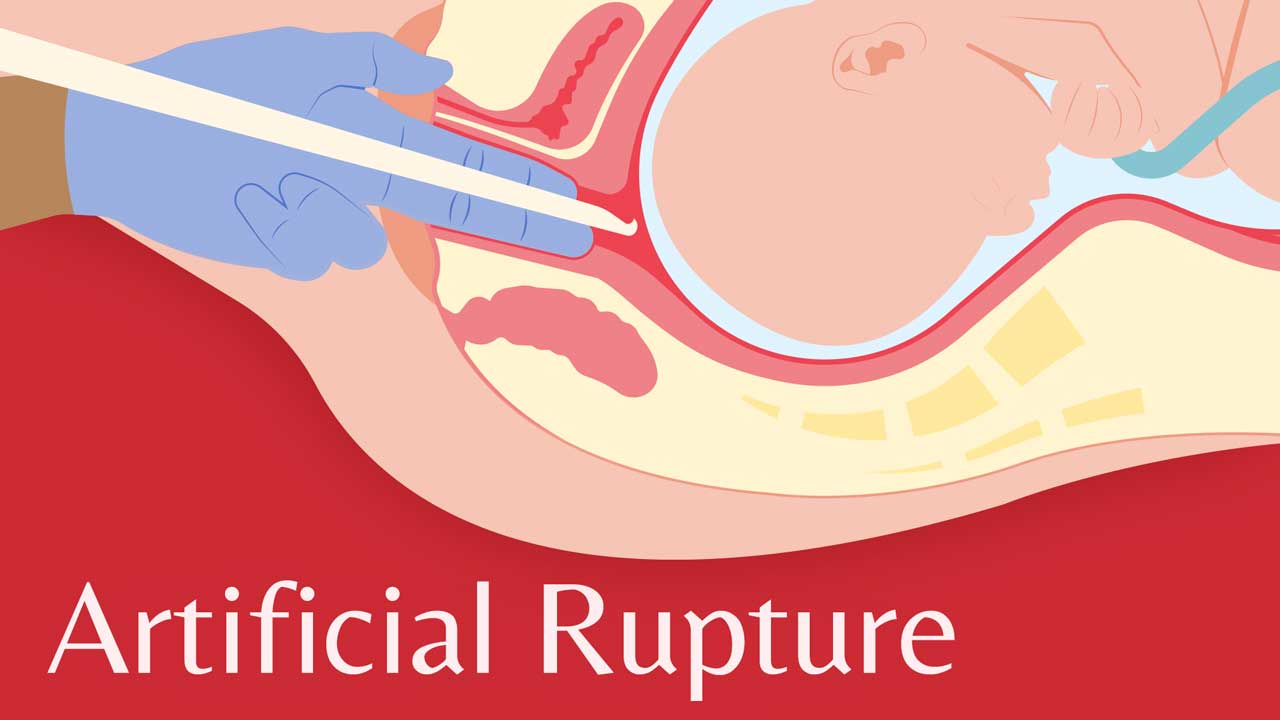
Artificial rupture of the amniotic membranes (ARM) is a method of inducing labour. It involves puncturing the membranes with a crochet-like, long-handled hook during a vaginal examination, releasing the amniotic fluid (RANZCOG 2021).
It is a simple procedure performed when the cervix is partially dilated and effaced, with the fetus in a vertex presentation with the head or other presenting part well-applied to the cervix to avoid prolapse of the umbilical cord (BHS 2019).
It’s thought that rupturing the membranes releases chemicals and hormones that can stimulate and speed up contractions and consequently shorten the length of labour (O'Connell 2021).
ARM may also be performed to allow the placement of fetal scalp electrodes if enhanced monitoring is required (Mahdy et al. 2023).
ARM may be used on its own or together with oxytocin therapy. If oxytocin is used, the fetus needs to undergo continuous cardiotocography monitoring (SCV 2023).
Note that ARM that can cause a significant increase in pain as the baby’s head will press directly on the cervix for the remainder of the labour (Cleveland Clinic 2022).

Although it’s commonly believed that ARM augments labour, there is limited evidence to support this, and data has shown mixed results. Despite this, ARM in conjunction with oxytocin has been shown to reduce the rate of cesarean birth if performed as an early intervention (Mahdy et al. 2023).
ARM might be performed to augment labour if:
ARM should not be performed if:
Risk factors associated with ARM include:

Perhaps one of the greatest arguments against ARM is that patients report it makes labour more painful. In a large study conducted by the National Childbirth Trust and reported on by the Royal College of Midwives (2012), 3,000 women were surveyed. The results were unequivocal with two-thirds of women reporting an increase in the rate, strength and pain of contractions following rupture of the membranes.
Not only did these women find their contractions more difficult to cope with, but they also needed more analgesia and felt that the physiology of labour had been disturbed, leaving them feeling less satisfied with their labour overall (RCM 2012).
After ARM is performed, the following will need to be monitored:
(Mahdy et al. 2023; Royal Hospital for Women 2020)